
July 16, 2026
When our plane landed in Dili, Timor-Leste, it was the only aircraft on the tarmac. We stepped directly onto the tarmac right by the runway and walked into an airport small enough to feel almost private.
At immigration, orderly queues formed around a handful of counters, which are only opened when one of the few commercial flights for the day lands. The infrastructure was bare, held together by some temporary-looking structures, but the process itself was linear and calm. That distinction stayed with me through the week, that institutions do not have to be grand, shiny or imposing to function well; ultimately, they are shaped by the people who make them work.
For the past year, part of the One Health Trust’s work as a World Health Organization (WHO) Collaborating Centre on Antimicrobial Resistance (AMR) has been to support the review of Timor-Leste’s National Action Plan (NAP) on AMR (2022-2026). Most of that work happened remotely, including reviewing policies and guidelines, studying public data, conducting interviews with officials and partners, and trying to understand how the country’s AMR response functioned through reports, documents, and datasets. This trip was about taking that work into the field to address the evidence gaps we had identified so far in our work.

An Aero Dili flight dropping passengers at the entrance of the terminal at Dili airport
A capital between mountains and sea
Dili is a small capital, framed by steep hills on one side and an expansive blue sea on the other. From the waterfront, the nearby island, Atauro, is visible on the horizon. It is a striking sight, but also a reminder of the practical realities of governing and delivering services in an island nation. Every public health system, supply chain, laboratory network, and vaccination program must extend beyond the capital and function across difficult terrain and sea crossings.
 Atauro Island, a separate municipality in Timor-Leste, viewed from Dili across the waters of the Wetar Strait
Atauro Island, a separate municipality in Timor-Leste, viewed from Dili across the waters of the Wetar Strait
Timor-Leste is still deeply connected to international support systems, and the changing global financing environment was a recurring thought throughout my week. Still, Dili never felt like a city defined only by its development partners. Portuguese and Indonesian influences were visible in language, food, architecture, and everyday life.
 A dinner with WHO colleagues in Dili
A dinner with WHO colleagues in Dili
Reviewing a national AMR response
The purpose of the mission was to support WHO and the Government of Timor-Leste in reviewing implementation of the country’s current AMR action plan, validating progress, identifying challenges and evidence gaps, and co-developing priority actions for the next phase of the national response.
Like much of fieldwork itself, this mission was also a learning experience, made richer by the opportunity to work alongside Dr. Sarah Paulin-Deschenaux from WHO headquarters and Dr. Bassem Zayed from WHO SEARO.
The review is organized around six themes: governance; coordination; monitoring and financing; awareness and education; surveillance data and use of evidence; prevention through infection prevention and control (IPC), water, sanitation, and hygiene (WASH), and immunization; access to and appropriate use of antimicrobials; and research and innovation.
Over two days, more than 80 stakeholders from across human health, animal health, fisheries, agriculture, environment, laboratories, hospitals, academia, and development organizations came together in a hotel in Dili to discuss and give their opinions on the findings. The workshop was less about presenting a finished analysis to the country’s officials involved in AMR-adjacent work, and more about testing our understanding against the experience these people who work within the system every day.
One of the most important messages to emerge was that Timor-Leste was building on already-strong foundations. The country has a national AMR strategy and is on the verge of being one of the first in the world to come up with its third five-year AMR action plan. It has treatment guidelines, an Essential Medicines List that incorporates the WHO AWaRe classification system (a framework that categorizes antibiotics into three groups—Access, Watch, and Reserve—to prevent AMR and optimize prescribing), a national laboratory system with growing technical capacity, and increasingly active engagement across sectors. There are dedicated people in ministries, hospitals, pharmacies, laboratories, and partner institutions trying to make these systems work.
But the central question throughout the week was how to turn systems that exist, many in policy or on paper, into systems that speak fluidly amongst themselves and function consistently at every level of care.
 The first day of the workshop in Dili
The first day of the workshop in Dili
Field Visits and Health System Realities
Some of the most important lessons came from outside the workshop rooms.
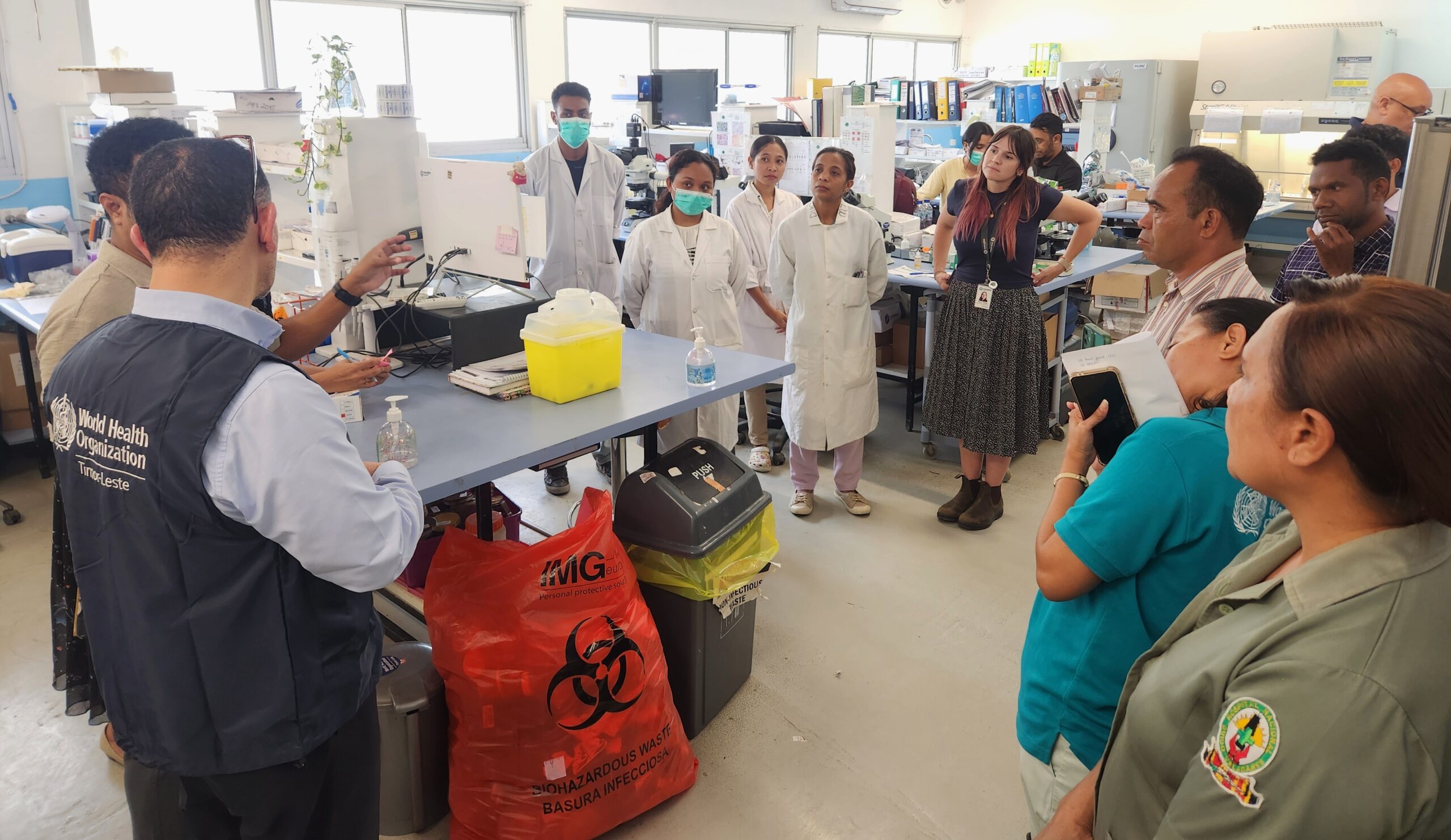
Midway through the mission, we visited primary and tertiary care facilities in Dili to better understand what AMR-relevant practices look like on the ground. We spent time with pharmacists, laboratory staff, clinicians, nurses, administrators, and infection prevention teams. We walked through pharmacies, general wards, specialized wards, delivery rooms, laboratories, and neonatal units.
At one primary care facility, there were important signs of progress. Pharmacists were familiar with the Essential Medicines List and appeared knowledgeable about AMR and appropriate antibiotic use. Medicine stock data were being entered into mSupply, the national medicine logistics system. Referral pathways for cultures and more advanced diagnostic testing existed.
But the limits of these systems were also visible. Handwashing stations did not always have running water or alcohol handrub or soap. Decontamination and waste-management systems required stronger attention. Stocks of essential medicines and diagnostic supplies were reported to be frequently interrupted. Many of the staff relied on WhatsApp groups for several important communications from laboratory tests to reporting stockouts.
WhatsApp had become a part of informal health-system infrastructure. It allowed messages to move quickly between clinicians, pharmacists, laboratory teams, and managers. In some cases, it was clearly useful, but a message sent was not necessarily a problem resolved. A complaint about a stockout might receive a quick reply telling someone whom to contact, without being formally logged or addressed or resolved at a higher level. It was an example of a wider pattern of ingenuity and responsiveness filling the spaces where formal systems were incomplete or insufficient.
One visit to the country’s only tertiary-care facility brought these questions home particularly sharply. In a neonatal unit, the density of incubators and the pressure on staff and space made infection prevention increasingly difficult. It was a vivid reminder that reducing infection risk is not only about having the right policy or protocol but also depends on whether there is room to work, whether essential supplies are within reach, and whether standard reporting processes are clear enough to follow under pressure.
I came away with many thoughts and a more grounded sense of what it means to write country-specific health policy recommendations from afar. A recommendation may be technically sound, but its value ultimately depends on the conditions that allow it to be practiced.
 Members of the visiting team in discussion with facility staff during a hospital
Members of the visiting team in discussion with facility staff during a hospital
Health System Capacity and Sustainability
The visit also revealed many opportunities and strengths, not just gaps. At the national health laboratory, we could see what sustained investment and strong technical partnerships can build. The laboratory has developed important capacity for microbiology, antimicrobial susceptibility testing, surveillance, and reporting. Hospital antibiograms are now being generated, helping clinicians and policymakers understand local resistance patterns and make better treatment decisions.
The laboratory system was one of the strongest parts of Timor-Leste’s AMR response that I encountered. But it also carried the familiar anxiety of sustainability. Much of this capacity has been built with financial support from external partners such as the Fleming Fund, with the technical assistance of partners such as Menzies. As donor funding changes or winds down, the question becomes not only how to expand these systems, but how to sustain what is already working.
This concern came up repeatedly during the mission. For a country that depends heavily on external financing, maintaining current levels of functionality can itself become an ambitious goal. Senior officials reflected on how some of the gains made during the COVID-19 period, particularly around infection prevention and control and health awareness, risk being lost as priorities and funding shift elsewhere. The ambition for the next phase of AMR work, therefore, is to merge priorities around building new systems while protecting and institutionalizing the systems that have already proven their value.
At the National Health Laboratory with colleagues from the Ministry of Health and technical partners
Working in a Small Health System
One of my most positive takeaways from Timor-Leste was the lack of cynicism I encountered. In larger country systems, it is common to hear good ideas dismissed quickly as too complex, too expensive, or politically unrealistic. In Dili, I found more willingness to ask if something could work there, and what that would take.
That may partly reflect the scale of the country. Over a single week, we could move from discussions with national leadership to conversations with hospital pharmacists, laboratory staff, municipal officials, and frontline health workers. The distance between policy and practice felt shorter in this setting.
That does not make implementation easy. Timor-Leste faces challenges in financing, transport, infrastructure, workforce capacity, and supply chains. But it does create a different kind of possibility. When decision-makers are reachable and systems are relatively compact, a well-designed policy recommendation can feel less abstract and more actionable.
A physical copy of the National Action Plan on AMR 2022-2026, the implementation of which is currently under review
The country’s senior officials also appeared to understand the bottlenecks clearly. They knew where supply chains were failing, where coordination was uneven, where laboratory systems needed support, and where prevention systems had weakened. The work ahead, hence, is more about creating the structures, accountability, financing, and political momentum to act on what is already known.

Dr. Sarah Paulin-Deschenaux and Dr. Bassem Zayed leading the field visit at a primary care facility in Dili
Going forward
The Timor-Leste mission was ultimately about more than reviewing a NAP. It was about understanding how a country can move from an important set of foundations toward a more functional, sustainable, and coordinated AMR response. The recommendations now being refined will feed into the next stage of national planning, potentially helping Timor-Leste shape a future NAP that is more closely tied to the realities of its hospitals, laboratories, supply chains, and communities.
For the One Health Trust, the mission also demonstrated the role a WHO Collaborating Centre can play beyond producing evidence: bringing together policy review, stakeholder engagement, field observation, and practical discussion about what comes next.
For me, it was a reminder that policy becomes real in very specific places: at a crowded neonatal ward, an empty hand-rub dispenser, a pharmacist’s Essential Medicines List booklet, a laboratory result sent over WhatsApp, or a room full of officials willing to ask how something might be done better. Those are the moments I will carry forward from Dili.










