
May 06, 2020
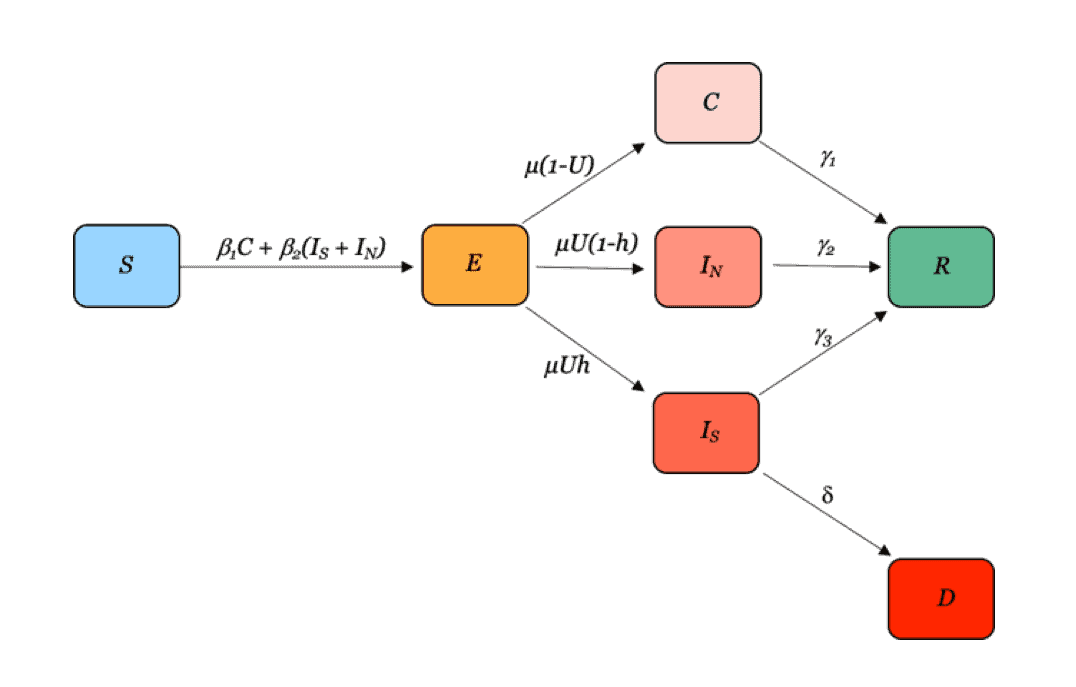
Here, we utilize a susceptible-exposed-contagious-infected-recovered, or SECIR, compartment model to estimate potential COVID-19 case burdens in each African nation considering various social distancing interventions.
The Question: Thus far, African countries have reported lower disease incidence compared to other regions. However, infectious disease surveillance and reporting infrastructure remain highly underdeveloped in many African countries, and COVID-19 testing is limited given the shortage of human resources and appropriate laboratory and surveillance facilities across the continent. Moreover, African populations may be at particular risk for high morbidity and mortality from COVID-19 given the high prevalence of immunocompromised individuals including those with HIV, malnutrition, and other communicable and non-communicable comorbidities. To contain the spread of COVID-19 and keep infections at a manageable level, many countries have instituted curfews, lockdowns, and other social distancing interventions. Effective implementation of such measures may be difficult to sustain given sociocultural, economic, and political challenges.
What We Found: Given current trends in case burden, the model estimates the potential resource needs that would be required under different scenarios. The model is for planning purposes and is based on current understanding and the most up-to-date assumptions. Results reported here are not forecasts but scenarios that may unfold given the assumptions about social-distancing and population health. Case estimates are provided for the following four scenarios:
- Baseline Disease continues to spread with no curfew, lockdown, social distancing, or other intervention(s) and with no change in transmission rate. (R0= 2.74)
- Intervention Scenarios:
- Moderate Lockdown Reduce transmission by 25% during lockdown period, then transmission resumes at 90% of pre-lockdown value due to sustained changes in behavior.
- Hard Lockdown Reduce transmission by 44% during lockdown period, then transmission resumes 90% of pre-lockdown levels.
- Hard Lockdown and Continued Social Distancing/Isolating Cases Transmission is reduced by 44% during the lockdown period then, through social distancing regulations and isolation of symptomatic individuals, resumes at 75% of pre-lockdown levels.
*As with all responsive research, this work has not been peer-reviewed. Current estimates are made using case data publicly available here. Our findings will be updated regularly to reflect best available data and insights on the SARS-CoV-2 virus and COVID-19 pandemic. This research was funded by the Centers for Disease Control and Prevention’s Modeling in Infectious Disease (MInD) Network and was produced by a team of researchers at CDDEP and John Hopkins University; this work does not represent the views of these institutions.
We present national case projections by African region according to the intermediate regional classifications set forth by the United Nations Statistics Division. (Inclusion/exclusion of a country or region and regional classification is meant for organizational purposes only and do not represent official endorsement or geopolitical position in any way.) National projections by region can be found below and will be continuously updated:
North Africa | Algeria, Egypt, Libya, Morocco, Sudan, Tunisia
Middle Africa | Angola, Cameroon, Central African Republic, Chad, Congo-Kinshasa (Democratic Republic of the Congo), Congo-Brazzaville (Republic of the Congo), Equatorial Guinea, Gabon, Sao Tome and Principe
West Africa| Benin, Burkina Faso, Cabo Verde, Côte d’Ivoire, Gambia, Ghana, Guinea, Guinea-Bissau, Liberia, Mali, Mauritania, Niger, Nigeria, Senegal, Sierra Leone, Togo
East Africa |Burundi, Djibouti, Ethiopia, Eritrea, Kenya, Madagascar, Malawi, Mauritius, Mozambique, Rwanda, Seychelles, Somalia, South Sudan, Tanzania, Uganda, Zambia, Zimbabwe
South Africa| Botswana, Eswatini, Namibia, South Africa
(*Comoros, Mayote, Reunion, Lesotho, and St Helena are currently omitted due to lack of case data.)
For comments or clarifications, please email Jessica Craig at [email protected]










